|
With my most recent CT scan continuing to show no sign of progression and my circulating tumor DNA tests showing no evidence of disease, my oncologist informed me that my Keytruda (pembrolizumab) infusions can stop at 36 (2 years). This first 7 infusions were part of 7 cycles of Padcev (enfortumab vedotin - 14 infusions) and Keytruda. This duration was determined in the KEYNOTE trials of Keytruda with various cancers including advanced urothelial cell carcinoma.
I began treatment on Dec 11, 2023 - 36 Keytruda infusions brings me to Dec 19, 2025. A nurse in the infusion suite said that they will miss me but will celebrate that day with me. Here's to a Merry Christmas after 14 more sessions in the chair.
7 Comments

  Blood drawn for laboratory work before my last infusion included samples for two circulating tumor DNA (ctDNA) tests - Natera Signatera and Northstar Response (discussed in my previous blog entry).
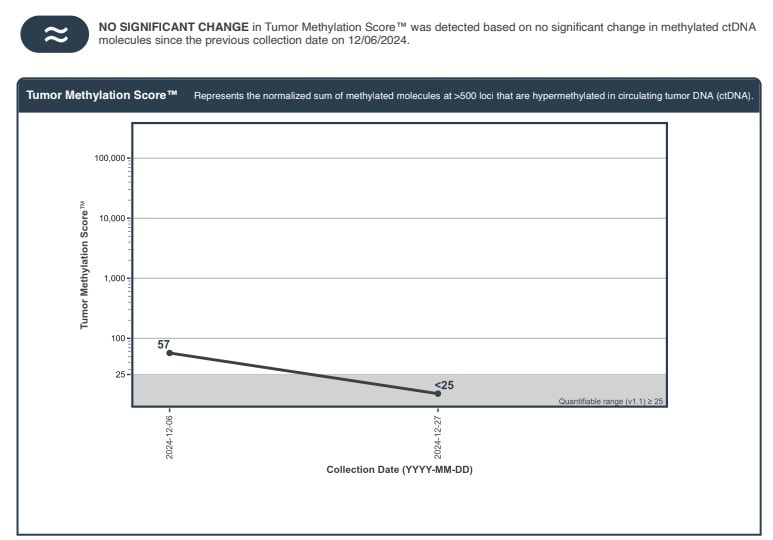
This is the fourth Signatera test (one roughly every 3 months ) that did not detect ctDNA. The Signatera test is based on genetic analysis of my tumor - looking for the DNA signature of my tumor and 16 likely mutations. The Response test looks for methylated DNA - a byproduct of cancer at work. It is estimated to have 10 times the "signal" of Signatera. My oncologist indicated that, because of it's sensitivity, he has seen changes even between cycles (every 3 weeks for me). I was encouraged to see that my second Response value was less than 25 and below its quantifiable range. This was not considered a significant change from my baseline (57). I will discuss with oncologist if I should draw blood for another Response test at my next infusion. I've also had a PET/CT scan which indicated that my lymph nodes were no longer active and two subsequent CT scans (all roughly 3 months apart) which showed no evidence of new metastatic disease. This surveillance data suggests to me I have had a complete pathological response (pCR) - as did 29% of participants in the EV302 trial, which led to approval of my treatment (enfortumab vedotin+pembrolizumab) as a first line option. I suspended enfortumab vedotin (Padcev) after 7 cycles due to adverse effects described previously. I've continued pembrolizumab (Keytruda) - 11 additional cycles so far. With my second Response test being consistent with my Signatera test - it raises the question of when I can safely suspend my Keytruda. pCR unfortunately does not mean that cancer is gone or will not recur. A recent article suggests that adjuvant immunotherapy should not be given to patients who exhibit pCR after neoadjuvant chemoimmunotherapy and surgery. The context is patients with resectable non-small cell lung cancer (NSCLC) - who receive a combination of immunotherapy and platinum-based chemo before surgery and demonstrate pCR after surgery. Results of recent trials suggest that pCR has a prognostic value for high event free survival (EFS). The authors note that the majority of patients (93% in the CheckMate-816 trial) who achieved pCR had no detectable ctDNA. They point out that an additional year of immunotherapy comes with risks of adverse effects and a financial cost (to insurer or patient). Given the encouraging results for patients who achieve pCR - they don't see the benefits outweighing risks in follow up immunotherapy. In my case surgery was my initial transurethral resection of the bladder tumor (TURBT) and chemoimmunotherapy was Padcev+Keytruda. My adjuvant immunotherapy is continuation of Keytruda. I believe that I have achieved pCR and will seek forums to pose the question (including discussing with my oncologist) of how long I should continue my immunotherapy and monitor the literature for any related guidance about continuing immunotherapy (unless and until I see recurrence of my disease).  It seems there is a name for approach I have been pursuing (and providentially led to) - risk adapted treatment for locally advanced muscle invasive bladder cancer: employing a systemic treatment - in my case enfortumab vedotin + pembrolizumab (EV/pembro or Padcev/Keytruda) - and active surveillance to determine if other treatment options are needed - which could include bladder removal (radical cystectomy) or chemoradiation (trimodality therapy). The results of a phase 2 trial following this approach were just published. The RETAIN-1 (NCT02710734) trial began 2016, before EV/Pembro was approved, and the neoadjuvant systemic therapy was AMVAC (accelerated methotraxate, vinblastine, doxorubicin and cisplatin). Genetic analysis was done on the tumors after transurethral resection of the bladder tumor (TURBT) looking for ATM, RB1, FANCC or ERCC2 mutations. After 3 cycles of AMVAC were completed and a second TURBT performed, patients with no residual disease and at least one of the listed mutations began active surveillance (AS). The end point of the trial was to be metastasis free survival IMFS) at 2 years for all enrolled. 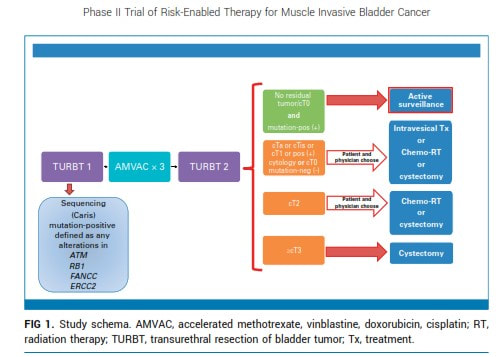 The end point was not met, however of the 25 patients enrolled in AS, 12 (48%) remained metastasis free with intact bladders at 2 years.
I began treatment with EV/pembro a bit more than a year ago. EV/pembro is an "all comers" treatment. EV delivers a chemothearpy payload to a Nectin-4 protein expressed on the majority of urothelial cancer cells and pembrolizumab blocks the PD-1 protein on immune cells to energize the immune system. Participants in the EV302 trial that led to EV/pembro approval were tested for PD-1 and Nectin-4. There was success (and some failures) for those with both high and low expression of both biomarkers. Therefore there is, at present, no biomarker to reliably select patients likely to have a positive response (which included a complete response for 29% of the participants in EV302). After 4 cycles of treatment, I had my first indication that I no longer had evidence of disease by PET/CT imaging and tumor-informed circulating tumor DNA (ctDNA). I've had two other surveillance data points, each roughly 3 months apart - CT scans showing no new metastases and no detected ctDNA by Signatera test. We suspended Padcev after 7 cycles and have continued with Keytruda. My oncologist told me of another ctDNA test - Northstar Response - which is tumor naive (not informed by analysis of my tumor). It looks for methylated tumor DNA - a byproduct of cancer at work - shed in the blood. The signal is potentially much higher and my oncologist has seen changes even between cycles (at the moment every 3 weeks for pembrolizumab alone). I drew blood for my first Northstart Response test on December 6 - the results are shown above. Not what I was hoping for, my baseline result indicates that there is still cancer there - low, but above the level where the value is too low to be certain. I drew blood for my second Response test on December 21 - where we can see if the trend is up, down or stable and plan action accordingly - again risk-adapted treatment. The baseline test also called out a CHEK2 mutation - which was also identified in my germline test (discussed in a previous post). The test also listed related clinical trials. NCT03375307 is clinical trial is a Phase II study evaluating the efficacy of olaparib (a PARP inhibitor) in treating patients with metastatic or advanced urothelial cancer that has DNA-repair defects (including CHEK2 mutation). I am reaching out to the investigators leading this trial to see if and when this might be a second line option if needed (restarting Padcev would be another option). Information is power and I know there is power in prayer and I plan to engage both. The weather, holidays and perhaps a bit of complacence have conspired to slow the pace of my exercise and periodic fasting - along with an increase in my weight and blood glucose. I will attend to these and while I wait on the next ctDNA results - prayers are always welcome.  I began treatment for locally advanced muscle invasive bladder cancer on December 15 last year.
Watching my sheep today reminds me of THE gift that secured my eternal destiny in a new creation free of disease. Until then my Christmas list... Complete response to new systemic treatments (e.g. antibody drug conjugates and immunotherapy) for locally advanced muscle invasive bladder cancer and others will be shown to be durable. AI will accelerate development and validation of better treatments. Biomarkers will be developed for accurate patient selection for these treatments. Molecular residual disease tests MRD (e.g circulating tumor DNA) will simplify surveillance and support prompt changes in management - including safe treatment de-escalation. Improved overall survival prognoses with preservation of quality of life (including bladder preservation) will be the norm. My fellow survivors will feel their Savior walking with them. WIshing all a joyful and blessed Christmas!  A recent publication caught my eye where a study was done with mouse models of and human patients with prostate cancer.
In the mouse models, the addition of white button mushroom (WBM) extract to the diet resulted in reduction in the number of myeloid-derived suppressor cells (MDSC) which promoted antitumor immune responses mediated by T cells and natural killer (NK) cells. They also observed increased anticancer activity of PD-1 antibodies In patients a decline was observed in the circulating MDSCs and increase in cytotoxic CD8+ T and NK cells. The City of Hope is recruiting for a phase 2 trial to further examine the effect of WBM on prostate cancer. MDSCs are also emerging target for bladder cancer. They contribute to the ability of tumors to evade immune detection. More research, such as that being pursied for prostate cancer, is needed to demonstrate the effect of reducing MDSCs in bladder cancer patients - however, the mechanism is the same for both. White button mushrooms offer a number of health benefits (including gut biome health and glucose control which I have mentioned elsewhere are of interest to me) and WBM extract is available as a supplement. My single treatment for muscle invasive bladder cancer at the moment is pembrolizumab - an immune checkpoint inhibitor. I've discussed with my oncologist and I am going to taking a daily dose of WBM extract to potentially enhance its effect. I will start with dose recommended on the product I ordered (500 mg - roughly 1/4 teaspoon daily). I may adjust as I learn more of the dose used in clinical trials. As always, with any change in diet or medication, you should consult with your care team. 1 year and 6 days ago I had my first PET/CT scan . [I've mentioned that I led software development for the first generation of PET/CT systems - but this was my first image as a patient.] That scan showed locoregional spread of my muscle invasive bladder cancer (MIBC) to nearby lymph nodes and changed the standard of care options - and the options would change again 35 days later with the FDA approval of enfortumab vedotin + pembrolizumab (EV/pembo - Padcev/Keytruda) as a first line option for locally advanced and metastatic MIBC. The performance in the phase 3 clinical trial (EV 302) that lead to approval was impressive - overall response rate of 67.7% and complete response rate of 29.1%. Testing was done looking at Nectin 4 expression (which enfortumab vedotin targets) and PD-L1 (which pembrolizmab targets) and both high and low groups showed had benefits in progression free and overall survival - therefore, no testing is required to begin EV/pembro treatment for locally advanced and metastatic MIBC. As I was seeing a good response - I was still curous if there were any explanation (beyond the power of prayer and God's grace) as to why. I requested a genetic analyis and received the report from a sample of my tumor resected 217 days earier. 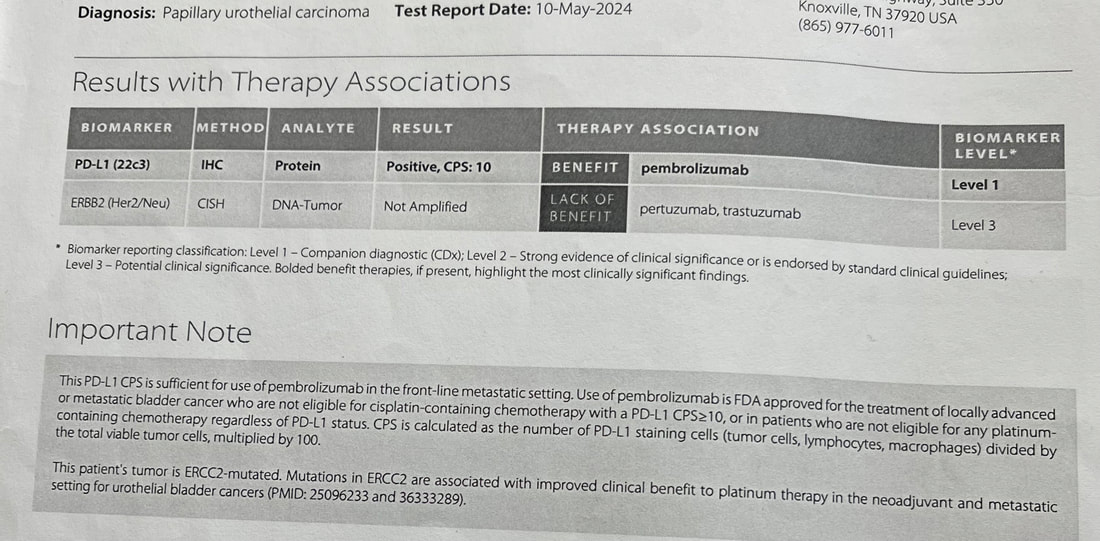 The report showed that I had a combined positive score (CPS) of 10 - which according to one study shows that I was likely to receive benefit from pembrolizumab. My tumor did not have FGFR mutations for which an FGFR inhibitor such as erdafitinib would be effective. A Nectin-4 histology score (H-score) could evalute its expression in my tumor cells. However, another study showed that a more common blood marker - C-reactive protein to albumin ratio (CAR) - can predict objective response to EV. 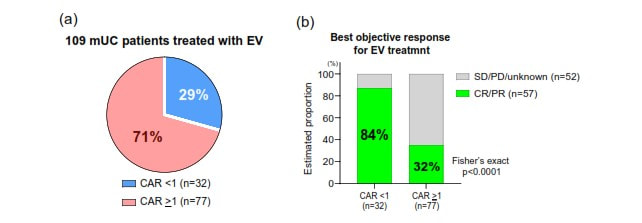 The results showed that lower CAR is associated with a better response. I am familiar with C-reactive protein (CRP) from a previous health journey (see earlier in the blog) where I lost 100 lbs and reversed type 2 diabetes. CRP is an indicator of inflammation - which is associated with type 2 diabetes. It may be that maintaing my weight, exercising and maintaining a low carb real food diet (including healthy fats and proteins) has resulted in a CAR <1 and contributed to a good response to EV. My lab work before each infusion includes an albumin measurement - I will ask to see if CRP can be measured as well to see if my CAR is below 1.
 In conversation with my oncologist I was made aware that there are clinical studies which show that a probiotic could enhance the performance of immune checkpoint inhibitors - which was of particular interest as I was now taking pembrolizumab (Keytruda) alone.
The probiotic used in the studies is Clostridium butyricum MIYAIRA 588 - a specific strain of anaerobic, butyric acid forming, Gram-positive bacterium isolated from a soil sample in Japan. Its primary use as a supplement is to regulate gut health (see the label above from the product I ordered from a supplier that imports from Japan). As documented earlier in my blog - 7 years ago, I began a low carb/high fat diet which, along with green exercise and intermittent and periodic prolonged fasting, was key to losing 100 lbs and reversing type 2 diabetes. I have maintained my weight and blood glucose by continuing to follow this regimen. CBM 588 is believed to modulate some potential gastroinstestinal side effects of a ketogenic diet, increase insulin sensitivity and optimize lipid metabolism. While more work needs to be done, in addition to bowel regulation, CBM 588 appears to be a good addition to my diet. What is most impressive for my current health journey are the results being reported when CBM 588 is used with immune checkpoint inibitors - specifically for renal and non-small cell lung cancer. The gut biome is known to play a key role in regulating the immune system. Imbalances, known as dysbiosis can lead to immune disfunction. In a phase 1b trial for renal cancer - the objective response rate (ORR) was 58% for those receiving immunotherapy and CBM 588, compared to 20% for those receiving immunotherapy alone. The immunotherapy was a combination of nivolumab (Opdivo) and ipilimumab (Yervoy). Nivolumab is a PD-1 checkpoint inhibitor like pembrolizumab (Keytruda). Ipilimumab targets the CTLA-4 receptor on T-cells. The improvements are consistent with the hypothesis that supplementation with CBM 588 works to reduce dysbiosis, support the immune system and improve efficacy of immune checkpoint inhibitors. A phase 1b trial examines safety - e.g. dosage and pharmokinetics. A phase 2 trial is planned to look at efficacy (as well as further examination of safety and optimal dosing). In the lung cancer study cited - 75% of the patients had a combination of chemotherapy and pembrolizumab. The addition of CBM 588 was associated with a longer overall survival and progression free survival. Less relevant for me, but interesting nonetheless - CBM 588 also been shown to be as effective against (non-muscle invasive) bladder cancer cells and potentially safer than the first immunotherapy BCG in in-vitro and in-vivo laboratory studies. I found a supplier of Strong Miyarisan, a supplement supplying CBM 588 on eBay (see label above). Each tablet contains 30 mg CBM 588. The recommended adult dose is 3 tablets 3 times per day or 270 mg. The dose administered in the renal cancer trial was 80 mg twice per day or 160 mg. I would welcome (and will lobby as I can for) a clinical trial of patients beginning a first line treatment of Padcev + Keytruda for locally advanced or metastatic muscle invasive bladder cancer - one arm supplemented with CBM 588 - the other without. This is the pathway that would allow doctors to prescribe CBM 588 as part of treatment. In the meantime, I am proceeding with the assumption that CBM 588 may boost efficacy of pembrolizumab. I am going to start with 2 tablets 3 times per day or 180 mg. As this supplement is considered safe, I believe that at a minimum I will have good intestinal health, likely benefits for my ketogenic diet (including insulin sensitivity and improved bowel health) and potentially improved efficacy of Keytruda fighting any cancer that remains. I will report any adverse effects. I currently have no evidence of disease by imaging or circulating tumor DNA and I am just one patient so it will be difficult to know if the addition of CBM 588 has been effective (or harmful) - I will continue to monitor any relevant trials. As with any decision affecting treatment - patients should discuss with their care team.  I received my third negative circulating tumor DNA (Signatera) test today. I discovered my disease - which turned out to be locally advanced muscle invasive bladder cancer (MIBC) - 390 days ago. I had a transurethral resection of the bladder tumor (TURBT) 15 days later and began treatment with enfortumab vedotin + pembrolizumab (EV/pembro or Padcev/Keytruda) 89 days after discovering the disease. The tumor sample was used by Natera to design my Signatera test to find evidence of residual disease by detecting tumor DNA shed into the blood from anywhere in the body. 3 months after my TURBT, 1 month after beginning treatment, I underwent an endoscopic procedure to remove and possibly replace a stent in my right ureter placed during the TURBT due to the tumor obstructing flow from my right kidney. The kidney flow was now brisk and there was no evidence of my primary tumor in the bladder. 84 days after beginning treatment (4 cycles) PET/CT now showed no significant uptake in my previously active pelvic lymph nodes or evidence of new metastatic disease. Two follow-up CT scans with contrast would also show no new significant findings. Given the good results, due to low grade adverse effects, we suspended the Padcev component after 7 cycles and have continued with Keytruda alone (currently 7 more cycles). Sensation in my fingertips and toes, sense of taste and hair have since returned. 29% of the participants in the EV 302 trial (that led to the accelerated approval of EV/pembro as a first line treatment for patients with locally advanced or metastatic muscle invasive bladder cancer) had a complete pathological response. I have no plans to pursue removal of or chemoradiation to the bladder. I am working to see that more high responders are followed to see how durable the response is. In the meantiume I hope to encourage more patients try EV/pembro as their first line treatment before pursuing radical cystectomy or bladder sparing with trimodality therapy. The vision was articulated by a leader in the field - Dr. Shilpa Gupta - at the recent EMSO 2024 meeting  I began my 7th cycle of enfortumab vedotin and pembrolizumab (Padcev+Keytruda) on May 31. I continued with pembrolizumab only on June 21. On September 13 I began my 6th cycle of pembrolizumab only. This is my second follow-up using CT with contrast since changing to immunotherapy alone. I would like to schedule a PET/CT and/or circulating tumor DNA to confirm - but I am happy to see a report of no evidence of recurrence or new disease by CT.
|
AuthorI began a health journey in the fall of 2017 - losing 100 lbs and reversing type II diabetes. Archives
March 2025
Categories |
 RSS Feed
RSS Feed