  Blood drawn for laboratory work before my last infusion included samples for two circulating tumor DNA (ctDNA) tests - Natera Signatera and Northstar Response (discussed in my previous blog entry).
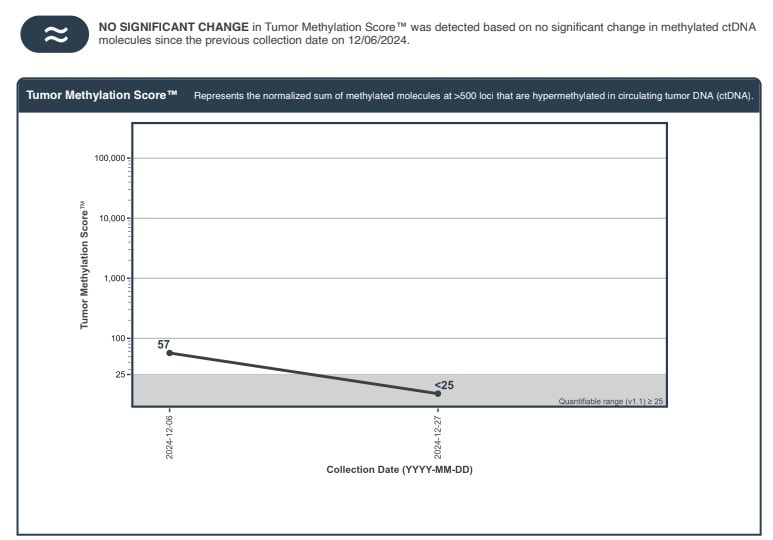
This is the fourth Signatera test (one roughly every 3 months ) that did not detect ctDNA. The Signatera test is based on genetic analysis of my tumor - looking for the DNA signature of my tumor and 16 likely mutations. The Response test looks for methylated DNA - a byproduct of cancer at work. It is estimated to have 10 times the "signal" of Signatera. My oncologist indicated that, because of it's sensitivity, he has seen changes even between cycles (every 3 weeks for me). I was encouraged to see that my second Response value was less than 25 and below its quantifiable range. This was not considered a significant change from my baseline (57). I will discuss with oncologist if I should draw blood for another Response test at my next infusion. I've also had a PET/CT scan which indicated that my lymph nodes were no longer active and two subsequent CT scans (all roughly 3 months apart) which showed no evidence of new metastatic disease. This surveillance data suggests to me I have had a complete pathological response (pCR) - as did 29% of participants in the EV302 trial, which led to approval of my treatment (enfortumab vedotin+pembrolizumab) as a first line option. I suspended enfortumab vedotin (Padcev) after 7 cycles due to adverse effects described previously. I've continued pembrolizumab (Keytruda) - 11 additional cycles so far. With my second Response test being consistent with my Signatera test - it raises the question of when I can safely suspend my Keytruda. pCR unfortunately does not mean that cancer is gone or will not recur. A recent article suggests that adjuvant immunotherapy should not be given to patients who exhibit pCR after neoadjuvant chemoimmunotherapy and surgery. The context is patients with resectable non-small cell lung cancer (NSCLC) - who receive a combination of immunotherapy and platinum-based chemo before surgery and demonstrate pCR after surgery. Results of recent trials suggest that pCR has a prognostic value for high event free survival (EFS). The authors note that the majority of patients (93% in the CheckMate-816 trial) who achieved pCR had no detectable ctDNA. They point out that an additional year of immunotherapy comes with risks of adverse effects and a financial cost (to insurer or patient). Given the encouraging results for patients who achieve pCR - they don't see the benefits outweighing risks in follow up immunotherapy. In my case surgery was my initial transurethral resection of the bladder tumor (TURBT) and chemoimmunotherapy was Padcev+Keytruda. My adjuvant immunotherapy is continuation of Keytruda. I believe that I have achieved pCR and will seek forums to pose the question (including discussing with my oncologist) of how long I should continue my immunotherapy and monitor the literature for any related guidance about continuing immunotherapy (unless and until I see recurrence of my disease).
2 Comments
|
AuthorI began a health journey in the fall of 2017 - losing 100 lbs and reversing type II diabetes. Archives
February 2025
Categories |
 RSS Feed
RSS Feed