 It seems there is a name for approach I have been pursuing (and providentially led to) - risk adapted treatment for locally advanced muscle invasive bladder cancer: employing a systemic treatment - in my case enfortumab vedotin + pembrolizumab (EV/pembro or Padcev/Keytruda) - and active surveillance to determine if other treatment options are needed - which could include bladder removal (radical cystectomy) or chemoradiation (trimodality therapy). The results of a phase 2 trial following this approach were just published. The RETAIN-1 (NCT02710734) trial began 2016, before EV/Pembro was approved, and the neoadjuvant systemic therapy was AMVAC (accelerated methotraxate, vinblastine, doxorubicin and cisplatin). Genetic analysis was done on the tumors after transurethral resection of the bladder tumor (TURBT) looking for ATM, RB1, FANCC or ERCC2 mutations. After 3 cycles of AMVAC were completed and a second TURBT performed, patients with no residual disease and at least one of the listed mutations began active surveillance (AS). The end point of the trial was to be metastasis free survival IMFS) at 2 years for all enrolled. 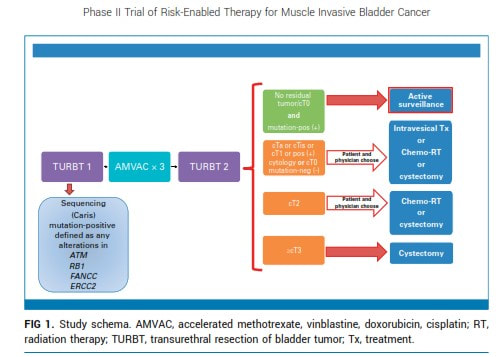 The end point was not met, however of the 25 patients enrolled in AS, 12 (48%) remained metastasis free with intact bladders at 2 years.
I began treatment with EV/pembro a bit more than a year ago. EV/pembro is an "all comers" treatment. EV delivers a chemothearpy payload to a Nectin-4 protein expressed on the majority of urothelial cancer cells and pembrolizumab blocks the PD-1 protein on immune cells to energize the immune system. Participants in the EV302 trial that led to EV/pembro approval were tested for PD-1 and Nectin-4. There was success (and some failures) for those with both high and low expression of both biomarkers. Therefore there is, at present, no biomarker to reliably select patients likely to have a positive response (which included a complete response for 29% of the participants in EV302). After 4 cycles of treatment, I had my first indication that I no longer had evidence of disease by PET/CT imaging and tumor-informed circulating tumor DNA (ctDNA). I've had two other surveillance data points, each roughly 3 months apart - CT scans showing no new metastases and no detected ctDNA by Signatera test. We suspended Padcev after 7 cycles and have continued with Keytruda. My oncologist told me of another ctDNA test - Northstar Response - which is tumor naive (not informed by analysis of my tumor). It looks for methylated tumor DNA - a byproduct of cancer at work - shed in the blood. The signal is potentially much higher and my oncologist has seen changes even between cycles (at the moment every 3 weeks for pembrolizumab alone). I drew blood for my first Northstart Response test on December 6 - the results are shown above. Not what I was hoping for, my baseline result indicates that there is still cancer there - low, but above the level where the value is too low to be certain. I drew blood for my second Response test on December 21 - where we can see if the trend is up, down or stable and plan action accordingly - again risk-adapted treatment. The baseline test also called out a CHEK2 mutation - which was also identified in my germline test (discussed in a previous post). The test also listed related clinical trials. NCT03375307 is clinical trial is a Phase II study evaluating the efficacy of olaparib (a PARP inhibitor) in treating patients with metastatic or advanced urothelial cancer that has DNA-repair defects (including CHEK2 mutation). I am reaching out to the investigators leading this trial to see if and when this might be a second line option if needed (restarting Padcev would be another option). Information is power and I know there is power in prayer and I plan to engage both. The weather, holidays and perhaps a bit of complacence have conspired to slow the pace of my exercise and periodic fasting - along with an increase in my weight and blood glucose. I will attend to these and while I wait on the next ctDNA results - prayers are always welcome.
1 Comment
 I began treatment for locally advanced muscle invasive bladder cancer on December 15 last year.
Watching my sheep today reminds me of THE gift that secured my eternal destiny in a new creation free of disease. Until then my Christmas list... Complete response to new systemic treatments (e.g. antibody drug conjugates and immunotherapy) for locally advanced muscle invasive bladder cancer and others will be shown to be durable. AI will accelerate development and validation of better treatments. Biomarkers will be developed for accurate patient selection for these treatments. Molecular residual disease tests MRD (e.g circulating tumor DNA) will simplify surveillance and support prompt changes in management - including safe treatment de-escalation. Improved overall survival prognoses with preservation of quality of life (including bladder preservation) will be the norm. My fellow survivors will feel their Savior walking with them. WIshing all a joyful and blessed Christmas! |
AuthorI began a health journey in the fall of 2017 - losing 100 lbs and reversing type II diabetes. Archives
June 2025
Categories |
 RSS Feed
RSS Feed