|
I recently participated in a spot for the American Cancer Society Cancer Action Network advocating for reimbursement of biomarker testing by insurers when deemed medically necessary. [I am continuing to support the ACS CAN as an advocate.] My lens was using circulating tumor DNA (ctDNA) to monitor my treatment response and status. The use and interpretation of ctDNA was topic of a number of presentations at ASCO. There is general agreement that ctDNA is prognostic (a good indicator of overall outcome) . It seemed that further studies are needed to develop guidelines for when and how ctDNA can be predictive - used in making treatment decisions. I had a chance to talk on the exhibition floor to fine representatives of the ctDNA tests I have used - Signatera (based on my tumor genetics described here) and Response (looking for methylated ctDNA, a general tumor marker described here). My first 4 Signatera tests were negative - I then had 3 Response tests. I learned at ASCO that a new Response assay was available with a 10 fold increase in sensitivity and that I would need a new baseline test moving forward. I drew blood for that test at my last treatment session.  I will need another test to see how my methylated ctDNA is trending. I, of course, would prefer to see my baseline Tumor Methlylation Score in the grey unreportable range (like my previous 2 tests with the original Response assay). The little man on my left shoulder whispers - "maybe there's still something there..." Although I side with the little man on my right shoulder - "the data supports a durable complete response and there's no evidence yet of residual disease" - it still brings to mind the question- "What WOULD I do next?" Here again - attending ASCO 2025 was informative... The first session I attended was - "Transforming the Battlefield: Targeting the Tumor Microenvironment" presented by Dr. Judith Varner. One tradition I appreciate greatly about ASCO presentations is putting the bottom line at the beginning and end as well as including a lay language slide.  The talk was germane to this post because it cited an example of enhancing response to immunotherapy in a second line treatment for advanced urothelial cancer (in this case first line treatment was platinum-based chemo without previous immunotherapy). They compared response of nivolumab (a PD-1 inhibitor like my immunotherapy agent pembrolizumab) alone to nivolumab and eganelisib. Eganelisib is a PI3K-gamma inhibitor which reprograms immune-suppresive macrophages in the tumor microenvironment. One of the immune suppresive agents affected are myeloid-derived suppressor cells (MDSCs). I take a supplement which has shown evidence of reducing MDSCs - it is described here. I also take a probiotic shown to improve efficacy of immunotherapy - it is described here. Studies of both of these supplements were performed at the City of Hope and I had a chance to stop by their exhibit and thank them for their work. 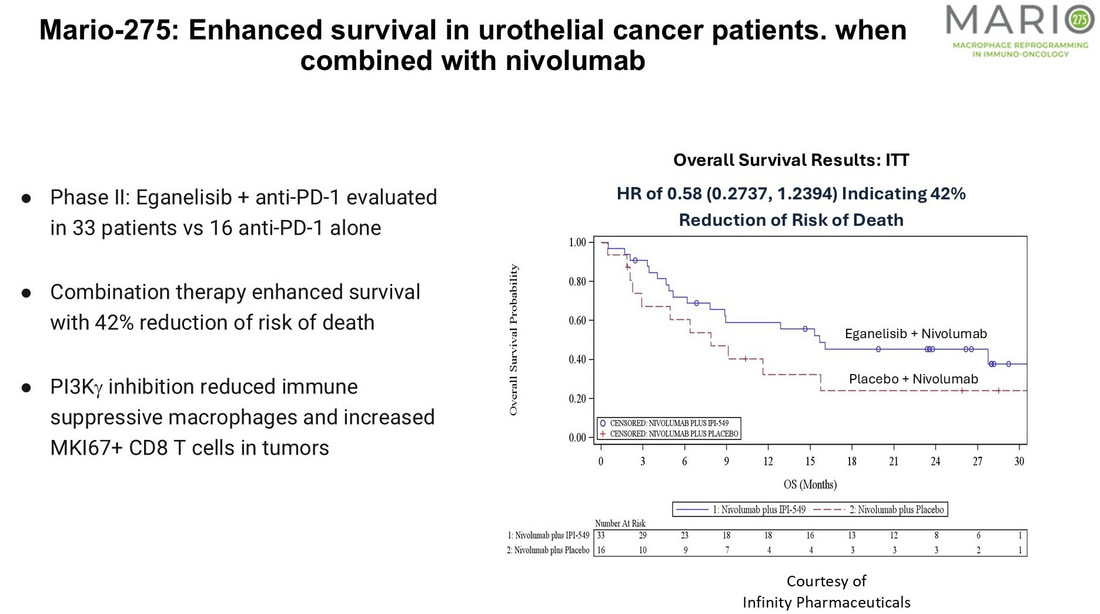 This was literally just the beginning, as progress continues to be made in antibody drug conjugates (similar to the enfortumab vedotin (EV) component of my first line treatment). My genetic analysis showed ERBB2 (Her2/Neu) and ERCC2 mutations with low Tumor Mutation Burden value of 8. [My germline genetic analyis found a CHEK2 mutation (discussed here).] I don't have FGFR2 or FGHR3 mutations (which eliminates agents targeting these mutations.)
In a session by Dr. Elizabeth Wulff - Antibody Drug Conjugates in Urothelial Carcinoma: Bridging Innovation and Community Practice, in addition to enfortumab vedotin (EV) - trastuzumab deruxtecan (T-Dxd), Disitamab vedotin (DV) and sacituzumab govitecan (SG) were discussed. T-Dxd is the first tumor agnostic ADC approved for HER2+ solid tumors (of various types) - but approval includes tumors having Her2 mutations like ERBB2. DV also targets Her2 mutations. In the RC48-C017 phase 2 trial, a pathological complete response rate (pCR) of 76.3% was reported for patients having HER2 expression of IHC1+ or higher. SG targets TROP2 (a protein which is overexpressed in many cancers including urothelial). Although accelerated approval for advanced MIBC was withdrawn in 2024, first results of the SURE-O2 trial presented by Dr. Andrea Necchi demonstrated a 44% confirmed clinical response (cCR) for SG in combination with pembrolizumab. Finally Dr. Shusuan Jiang presented results from a phase 1b/2 study of Bulumtalug Fevodotin (BFv) and Toripalimab. BFv, like EV, targets the Nectin 4 protein and Toripalimab is an anti-PD-1 monclonal antibody (similar in action to pembrolizumab but with potential advantages). Treatment naive patients saw a confirmed objective response rate (cORR) of 87.5%. It may offer better efficacy and tolerability than my first line treatment (EV+pembro). Although EV+pembro represents the new standard of care for first line treatment - my ERCC2 mutation indicates that I should be responsive to conventional platinum-based chemotherapy. There are also other developments on the horizon (bi-specific antibody drug conjugates and bicyclic peptide drug conjugates) which may be evaluated soon in clinical trials. Bottom line - it seems that I have a fine lineup of (bladder sparing) therapuetic options waiting should my cancer recur. That's not my expectation - but I will be prepared to discuss with my excellent care team. P.S. After I posted this entry on June 25 - I found an expert view of exactly this question here. It was presented on June 27 by Dr. Tom Powles at the Guard Symposium in Madrid! I was reminded that I neglected to mention that rechallenging with EV is also an option. I suspended EV after 7 cycles due to low grade adverse effects and a cCR.
0 Comments
Leave a Reply. |
AuthorI began a health journey in the fall of 2017 - losing 100 lbs and reversing type II diabetes. Archives
June 2025
Categories |
 RSS Feed
RSS Feed